.svg?sfvrsn=be606e78_3)
- Home
- The Magazine
- Article
OR Excellence Awards: Pain Management: Less Pain With Bupivacaine
By: Adam Taylor | Managing Editor
Published: 9/5/2024
Share:
Implants get patients home faster and keep them safe once they get there.
Postoperative pain is a common symptom after inguinal hernia repair, with patients still reporting pain even after being discharged home.
Long-acting extended-release anesthetics used in combination with other non-narcotic pain medication as a multimodal pain management strategy are helpful. These alternative medications offer advantages, including prolonged control of incisional pain, decreased narcotic usage and reduced time spent in the PACU.
These medications are not without danger, however, as they pose a risk for patients developing local anesthetic systemic toxicity (LAST) syndrome. LAST is caused by the accumulation of the components in these medications, and the blood level of local anesthetics can last up to 96 hours after administration.
Patients receiving these alternative medications intraoperatively are at risk of LAST throughout all phases of care and even afterward when home. The Hospital of the University of Pennsylvania in Philadelphia not only found a way to reduce the risks of LAST in hernia patients, but the facility also simultaneously decreased postoperative pain scores and lengths of stay in the PACU. For those reasons, the Penn Medicine Hospital of the University of Pennsylvania in Philadelphia was awarded the 2024 OR Excellence Pain Management Award.
The team used a long-acting bupivacaine-impregnated collagen implant to achieve these goals. Prior to implementation, the patients’ average length of stay in the PACU was 159 minutes and the average pain score reported was 3.97 out of 10 on the Edmonton scale. Once the new implants were used, the average PACU length of stay was reduced by 33 minutes to 126 minutes, a 20% reduction. The average reported pain score was reduced, from 3.97 to 1.77 on the scale.
Honorable Mention: IV-START IMPROVEMENT
Repurposed Ultrasound Machine and New Training Program Get Results
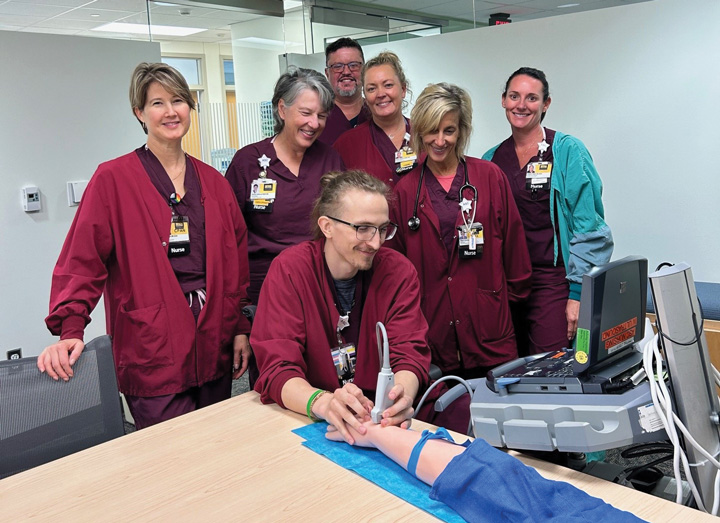
SOUND GUIDANCE The team at University of Iowa Healthcare’s ASC uses a training arm to practice ultrasound and IV-start skills. | University of Iowa Healthcare
The 5% of patients at University of Iowa Healthcare’s Iowa City ASC who were the recipients of at least three IV start attempts before a line was placed successfully certainly weren’t happy about it, and neither was the staff. The difficulty resulted in delays in starting procedures in some cases.
An ultrasound machine that wasn’t in use was located in the system, which the staff acquired and created a training module and rating sheet. A QR code was used to collect data on how many times the ultrasound machine was used and how successful it was.
The number of cases in which more than three IV attempts were needed decreased from 5% to 2.5%. The number of times an anesthesia provider needed to start an IV after a nurse had tried decreased from 6% to 0.8%. Patient satisfaction scores about nurses’ skill for starting IVs increased from 82% to 85% in the first month of the project.
Thirteen nurses were trained and there are plans to buy another ultrasound machine and train more nurses, says Nurse Manager Donna Dolezal, RN, MSN, CPAN, CAPA.
“I’m very proud of how the frontline team stepped up to be champions for our patients and reduce the number of multiple IV placement attempts,” adds Associate Director Molly Kucera, MBAHC, BSN, RN, CNAMB, CNOR.
—Adam Taylor
“Patients also reported pain control post-discharge and infrequent use of opioids on post-procedure phone calls,” says Ann Marie Morris, MSN, RN, CNOR, CSSGB, associate clinical director of perioperative quality and safety. The quality improvement group included nursing representatives, as well as a surgeon, anesthesiologist, pharmacist and IT representative.
“It was crucial that the care team understood the risks and benefits to patients while under our care and that discharged patients were still at risk for LAST for 96 hours,” says Ms. Morris. “Our care team partnered with IT to create electronic medication documentation that triggered an interface to the procedure-specific discharge instructions, alerting the patient that they received this medication.”
Also, an alert bracelet is placed on all patients, who received these medications intraoperatively. Patients are discharged with this bracelet indicating the medication received and the exact time the restriction ends. OSM
Honorable Mention: DRASTIC OPIOID REDUCTIONS
Nerve Blocks and Multimodal Analgesics Solve an Overprescribing Issue for Cancer Surgery Patients

TEAMWORK Cancer surgery patients go home with fewer opioids thanks to quality improvement work by the staff at Josie Robinson Surgery Center in New York City.
Patients at Josie Robertson Surgery Center, a freestanding facility of Memorial Sloan Kettering Cancer Center in New York City where same-day surgeries are performed, need their pain controlled for a quick discharge while remaining on a pathway that allows them to actively participate in their post-op education and recovery programs.
Realizing that overprescribed opioids presented a barrier to those goals, the facility’s quality improvement team created a program that worked. Before the project, the standard median prescription at discharge was for 20 pills — even though the median consumption was only two pills.
“Opioid prescriptions were later standardized to 7, 8 and 10 pills in the gynecology, urology and breast services respectively,” says Aimee Dannaoui, MSN, RN, NE-BC, CAPA, the facility’s director of nursing, ambulatory surgery and perioperative services.
The facility’s successful use of regional nerve blocks and multimodal analgesics played a big role in the reduction of opioids needed for post-op pain control. The reduction in prescribed opioids at discharge was not associated with an increase in reported pain, and the center maintained its more than 95% patient satisfaction scores.
“We remain proud and committed to our high standard of care, patient safety and patient satisfaction in the ambulatory setting, putting our patients and their community at the forefront of our care,” says Ms. Dannaoui.
—Adam Taylor
.svg?sfvrsn=56b2f850_5)