.svg?sfvrsn=be606e78_3)
- Home
- Article
The Staples of Successful Wound Care
By: Kimberly Jones, DNP, RN, CNOR, RHCNOC
Published: 3/7/2023
Share:
Closing surgical sites properly and managing incisions post-discharge are the critical final steps of satisfactory surgeries.
Successful wound care is about staying true to the basics. Not every surgical wound will need an antimicrobial dressing or wound vac. But paying special attention to closing every surgical site properly, carefully managing incisions post-discharge and providing patient education are always the necessary ingredients for successful surgeries as well as safe and happy patients.
At Ascension St. Vincent Mercy Hospital, we pride ourselves on our wound care. Here’s how we incorporate negative pressure wound therapy, antibacterial dressings and irrigation into our wound care protocols.
Methods worth mastering
There are several wound care methods that surgeons utilize in the OR to stimulate healing and prevent infections, including:
• Negative pressure wound therapy. Also known as vacuum-assisted closure (VAC), this alternative method of wound management uses negative pressure to prepare a wound for natural healing. Negative pressure wound therapy is great for wounds that have difficult healing, such as diabetic ulcers, wounds that are difficult to close and wounds surrounded by excess adipose tissue.
We’ve utilized disposable wound vacs for our total joints patients who have a larger amount of adipose tissue. The system helps to keep them as clean and dry as possible. For our podiatry and general cases, we utilize a reusable system that comes with a portable canister that patients carry around. Pieces of foam dressing get packed into the wound and then a clear waterproof dressing goes over the foam to create a complete seal all the way around the wound. Once you have that perfect seal, you connect tubes to a portable canister to collect any drainage. There is often a large amount of drainage with our podiatry and general cases, which is why the canister is necessary.
Application of a reusable wound vacuum system is tedious and detailed. It’s really important to count and document the number of sponges that go into the wound before you close the dressing. This ensures whoever takes off the dressing knows exactly how many sponges were used and how many need to come out.
In the past, we’ve seen instances where a sponge count wasn’t done, and the patient had a significant wound infection, resulting in a return to surgery — all because sponges weren’t removed. It’s also important that the sponges are changed every two days by someone with extra training in wound management. Every once in a while, a patient will go home and their wound vacuum will start leaking or they’ll lose the pressure in their dressing. That’s why we educate both the patient and their caregiver on the importance of maintaining that dressing and what to do if it stops working. If a leak occurs or the vacuum loses suction, patients and caregivers leave our facility with the understanding that the dressing must come off within two hours. Anything longer than that and bacteria will start to grow, which sets them up for an increased risk of infection.
• Antibacterial dressings. These products in-clude antiseptics such as silver, cadexomer iodine, polyhexamethyl biguanide (PHMB) and medical grade honey to reduce the load of a variety of pathogens. Antibacterial dressings look like giant Band-Aids that seal all the way around and are waterproof.
We don’t utilize these dressings much in our OR — except when we want to apply an occlusive dressing to the patient’s incision so they can shower. We do, however, use these dressings frequently in our wound care clinic. Depending on the patient, wound and amount of drainage, the dressings can stay on for up to a week or be changed a couple times weekly.
• Wound irrigation. The old adage, “The solution to pollution is dilution,” is what always comes to mind. Every surgeon has their own preferences and irrigation techniques. Some prefer to use saline, while others choose to mix antibiotics in their irrigation or rely on a povidone-iodine or a chlorhexidine gluconate (CHG) solution. Although there is no standard practice recommendation, we’ve found great success using a CHG-based solution in several different types of cases, from general surgery to orthopedics. For our podiatry cases, we use a system that is similar to a pressure washer. It debrides while it irrigates and helps to create a clean wound bed that will speed healing.
Patient prep
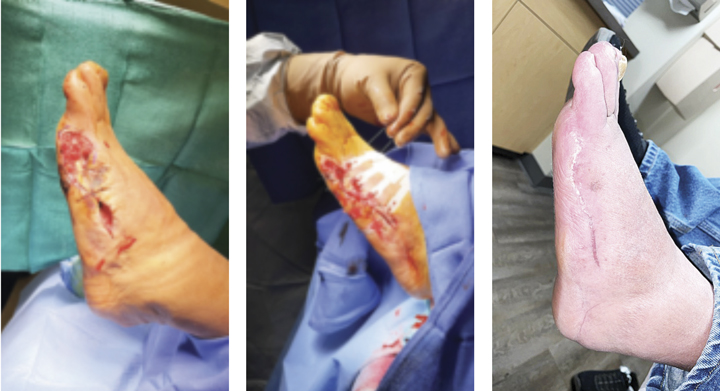
STAGES OF HEALING Techniques used on this patient included a multistaged approach with repeated debridement, skin adhesives and negative pressure wound therapy. | Nathan Graves
Your surgical team may be unapologetic about the high standards they hold to prevent surgical site infections (SSIs), but if the patient doesn’t receive proper training on how to care for their wound, those standards go right out the window. Patient education begins during their pre-op interview, which takes place about a week before the scheduled surgery. We stress the importance of taking a shower the night before and morning of surgery. For certain cases, a shower with a CHG-based soap is necessary. We also tell patients to arrive for surgery in clean clothes with their teeth brushed. When they arrive, we talk to them about what they can expect during surgery, what they can expect afterward, how important it is to maintain their dressing, when they can remove the dressing and how to keep it clean. Post-op, we go over the instructions again with the patient and their caregiver. When they leave the hospital, we provide them with detailed written instructions. Finally, we call the patient post-op — usually 48 to 72 hours after their surgery — to check on them, make sure they’re doing well and that they’re happy with their care. Then, we go over their wound care with them yet again, making sure they don’t see any signs of infection.
When choosing the best wound closure method, it’s vital surgeons take into account anything and everything that might affect that wound. This means considering every bit of how that dressing will affect that particular patient. For example, my orthopod will glue incisions shut on his shoulder patients, because a big, bulky dressing on a shoulder is uncomfortable and the glue allows the patient to shower sooner. You should also take into consideration the patient’s home life. Some patients are cleaner than others and there are some who simply won’t take extra precautions to make sure their surgical site stays as clean as possible while it heals.
No shortcuts to safety
We’re a critical access hospital in central Indiana, and we’re honored to care for some very sick patients as well as perform general surgery, orthopedic, podiatry, ENT and urology cases in our two OR suites.
Our surgical services team at Ascension St. Vincent Mercy Hospital is proud and unapologetic about the high standards that we hold. By refusing to waver on these patient care expectations, our team is now into year four with zero SSIs.
Of course, wound care is just one piece of a comprehensive SSI prevention puzzle that begins with instrument reprocessing and ends by closing surgical sites properly and managing incisions post-discharge. We refuse to take shortcuts when it comes to patient safety. OSM
.svg?sfvrsn=56b2f850_5)