.svg?sfvrsn=be606e78_3)
- Home
- Article
Pressure Injury Prevention and Treatment Essentials
By: Carina Stanton | Contributing Editor
Published: 11/26/2024
Share:
A dedicated mindset and bundled prevention practices can be the one-two punch needed.
Traditional thinking about pressure injuries (PIs) can lead to many providers only being on guard against them when caring for older patients in acute-care settings who have mobility issues or comorbidities that influence their vascular health.
But smart OR teams know there’s more to the story — even in same-day surgery centers.
That’s why comprehensive PI prevention practices, which include risk assessments, improved dressings and better handoffs, are now considered appropriate for the majority of surgical patients in outpatient settings. Recent research has found pressure injuries are one of the top reasons for delayed postoperative recoveries across varied patient populations.
Recognizing surgical PI risks
Evidence-based guidance from organizations such as the Association of periOperative Registered Nurses (AORN), the National Pressure Injury Advisory Panel and The Joint Commission spell out two main reasons most surgical patients are at risk for PIs.
First, the immobility required for surgery alone is a risk factor. Second, surgical patients are often less mobile prior to an elective surgery for a repair such as a joint replacement. As a result, many outpatient surgery centers riding the total joints wave are paying closer attention than ever before to PI risk scores.
There’s another risk, however: a lack of attention among providers toward PIs, notes Kate Wolf, MSN, RN, CNOR, OR education coordinator at the Clement J. Zablocki Veterans Affairs Medical Center in Milwaukee. “Pressure injury prevention can easily get overlooked during the hustle and bustle of a busy case,” she says. “Over time, it starts to lack importance, and the patients are the ones who end up suffering when a pressure injury occurs.”
Reducing surgical PIs
Ms. Wolf works on many fronts to raise awareness about surgical PIs, both on macro and micro levels. She has served on AORN’s Guidelines Advisory Board and has worked closely with the association’s senior director of perioperative evidence-based practice, Lisa Spruce, DNP, RN, CNOR, EBP-C, CNS-CP, ACNP, ACNS, FAAN, the lead author of AORN’s Guideline for Prevention of Perioperative Pressure Injury. Meanwhile, in the ORs at her facility, Ms. Wolf has worked with staff nurses Rachel Labinski, BSN, RN, and Chelsea Gruettner, ADN, RN, to successfully reduce PIs in surgical patients.
Ms. Wolf, Ms. Labinski and Dr. Spruce agree that there are four key essentials to successfully prevent and treat pressure injuries. They boil down to this: change the culture around PIs, bundle practices, discuss PI risk and incidence, and support postoperative recovery. Let’s dive into each.
1. Create a perioperative pressure injury prevention program
Changing hearts and minds about the risks of pressure injuries requires consistency and collaboration. A dedicated perioperative pressure injury prevention program is an effective way to instill a fresh cultural mindset for PI prevention, according to Dr. Spruce.
She says the program should be led by an interdisciplinary team of nurses, physicians, wound care experts, quality experts, leadership and others who have the authority and responsibility to develop policies and procedures for preventing perioperative PIs — with assessments being a key focus for standardization.“When teams have standardized pressure injury prevention risk assessments and skin assessments woven into practices for every patient, pressure injury prevention goes from being a marginal focus to a central care focus, and that is the true key to prevention,” says Dr. Spruce.
2. Develop a PI prevention bundle
Ms. Wolf and Ms. Labinski worked with their organization’s perioperative PI prevention team to create and implement a bundled approach that has proven effective.
In 2022, the first year of the bundle’s implementation, surgery-induced PIs declined from 17 to five in the first six months, with only two occurring in the next six months. In 2023 and so far in 2024, there have been zero potentially preventable PIs at the facility. The bundle they developed drives that success, they say. It is built around three elements: a PI risk assessment, proper use of dressings and pressure reduction devices, and effective communication about the PI risks of the patient during hand offs.
• Assessments. “Assessments are essential because interventions will be implemented to prevent pressure injury and those interventions will be determined by the risk assessment,” says Dr. Spruce. “Facilities should conduct a preoperative assessment of every patient’s risk for PI as part of the routine assessment of their patients and part of the standard of care for all patients. Based on the outcome of the risk assessment, they would implement interventions to prevent a PI.”
Dr. Spruce notes that length of surgery, a commonly acknowledged factor, is only one of numerous PI risk factors providers must consider. She additionally recommends a structured, age-specific PI risk assessment tool be used to capture a wider range of patient-related and procedure-related PI risks. Validated assessment tools recommended in the AORN guideline include the Munro Scale, The Risk Assessment Scale for Perioperative Pressure Injuries (commonly known as ELPO), the Perioperative Risk Assessment Measure for Skin (PRAMS) tool and the Scott Triggers tool.
Ms. Wolf’s and Ms. Labinski’s preoperative teams use the Scott Triggers assessment. If it reveals that the patient is a positive risk for PIs, the PI prevention bundle is implemented. The preoperative nurse always documents the patient’s Scott Triggers score in the electronic health record.
• Dressings and pressure reduction devices. AORN recommends that prophylactic materials such as dressings or non-adherent PI prevention devices be applied to bony prominences including the heels, sacrum and other areas subjected to pressure, friction and shear in high-risk patients. These patients should also be placed on high-specification reactive or alternating air pressure support surfaces, says Dr. Spruce.
When a patient’s risk assessment score identifies high risk at Ms. Wolf’s and Ms. Labinski’s facility, they get bilateral heel and sacral antimicrobial foam dressings. The patient’s Scott Triggers score is discussed during the hand off before surgery, as are the skin assessment and any preoperative interventions that were implemented. Once the patient is in the OR, the intraoperative team determines if there is a need for further PI prevention interventions, including positioning aids, foam padding or additional antimicrobial foam dressings.
• Communication across care teams. All of the necessary communication among provider types during the PI prevention process should be standardized and followed consistently at all levels of perioperative care, says Dr. Spruce.
Because Ms. Wolf and Ms. Labinski work at a teaching facility, every case can involve a variety of residents, fellows, medical students and attending surgeons. With so many different individuals involved in surgeries, effective standardized communication is exceptionally crucial to ensure that all measures for PI prevention are followed. The OR nurse documents all interventions in the electronic health record, and after the surgery is complete, the OR nurse conveys to the PACU nurse the interventions and skin condition of the patient during the hand off, says Ms. Labinski.
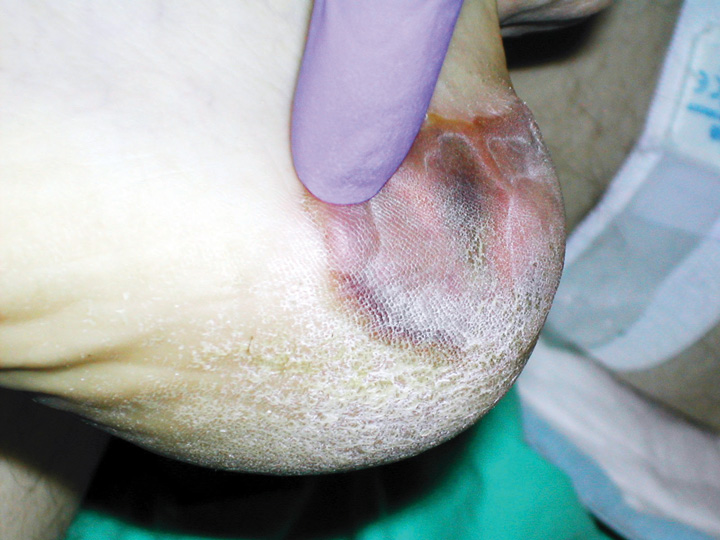
RUBBED RAW Pressure injuries often occur in vulnerable areas and, despite misconceptions to the contrary, happen in both inpatient and outpatient settings.
“Every hand off in perioperative services includes a discussion about patient skin on arrival, interventions used, and any areas to watch out for,” says Ms. Wolf. “For example, if the patient was prone, even though their incision is on their back, the chest needs to be monitored as well.”
3. Keep talking about the issue
Effective incident reporting can help teams refine processes and protocols to better address and reduce PIs. Dr. Spruce advises that root cause analyses to determine the etiology of PIs are essential. These reports and analyses should be communicated throughout the perioperative care team.
When a PI has developed postoperatively in a patient at Ms. Wolf’s and Ms. Labinski’s facility, a wound nurse tracks and investigates the case. They start by contacting the OR nurse who cared for the patient. Next, the wound nurse has the OR nurse complete an audit form to document all aspects of the procedure to try to determine how the PI developed and how it could have been prevented. The findings are presented to the facility’s pressure injury prevention committee, as well as the OR team at a staff meeting.
“By engaging staff in the process and discussing the importance of skin as a part of every hand off, more focus is being given to the skin condition and protection interventions overall,” says Ms. Wolf.
4. Prepare patients for PI-free recoveries
Ms. Wolf suggests three home-care strategies that can help patients and caregivers prevent postoperative PIs:
First, encourage the patient to shift their weight at least every two hours. Caregivers should be close by to assist with turns if needed. If the patient had a previous pressure injury, that area will be more prone to break down and requires more frequent and thorough monitoring.
Second, if the patient has limited sensation, the caregiver should ensure the patient’s sheets don’t have wrinkles, and that water and heat packs are at appropriate temperatures.
Finally, the patient should be consuming enough protein and vitamins to help with wound healing and prevent any possible tissue breakdown from the stress of the procedure.
Every patient, every time
One thing is clear: your facility’s strategy for prevention of pressure injuries should not be a matter of individual provider preference or routine. It requires communication throughout the team, and an appreciation that every surgical patient is an individual who requires an individual assessment and prevention plan based on solid evidence-based protocols to which the entire perioperative team adheres. OSM
.svg?sfvrsn=56b2f850_5)