.svg?sfvrsn=be606e78_3)

Numbing nerves with local anesthetics relieves post-op pain for days at a time. Freezing them with a blast of targeted cold therapy can provide the same soothing effect for weeks or even months. "Cryoanalgesia has the potential to reduce the reliance on traditional opioid-based pain management strategies," says Jon Wilton, DNAP, CRNA, chief nurse anesthetist at Mercy Medical Center Mt. Shasta (Calif.). "Limiting opioid use reduces associated side effects, including addiction, and facilitates early post-op mobility."
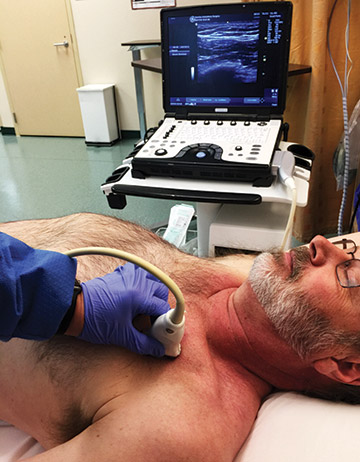
Cryo is performed percutaneously by guiding a closed probe next to a nerve. Carbon dioxide or nitrous oxide is passed through the probe until the gas reaches the probe's tip and the pressure drops, which results in a drastic cooling. The end result is the creation of an ice ball that encompasses the targeted nerve, freezes and disables it, and keeps patients pain-free for extended periods.
The potency of this pain-relieving treatment is one of the major reasons facilities are increasingly looking at cryo in their quest to improve patient comfort with fewer opioids. It's also why the treatment is beginning to pique the interest of surgical professionals who want to advance the management of post-op pain with longer-lasting analgesia.
.svg?sfvrsn=56b2f850_5)