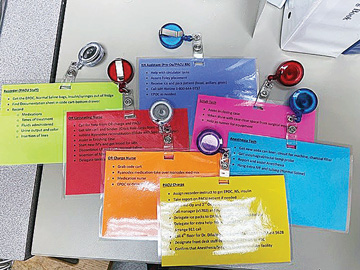
The beauty of the role cards is they list all the specific duties each team member is required to complete during an MH emergency. This not only allows for optimal coordination, but it also provides staff with an easy-to-access reminder of the
facility’s response protocols. If a team member gets flustered or goes blank on their responsibilities, all they have to do is look to their cards for answers. While every facility will have their own twist on creating role cards, here
is how we broke down the responsibilities for each team member during an MH crisis:
• Circulating nurse. The circulating nurse must call for help from the OR or the PACU and immediately grab the MH cart and binder. (We keep the role cards in the front pocket of the binder for easy access.) They should then initiate
dantrolene reconstitution, assist in securing the patient, start new IVs as needed and get blood samples for labs. The circulating nurse should also discontinue the use of Lactated Ringer’s solution (LR) and start the patient on normal
saline. They should also insert the Foley catheter to monitor urine color and flow, and delegate important tasks as needed.
• OR charge nurse. The OR charge nurse’s first task is grabbing the code cart and diluting dantrolene with sterile water. This nurse is also responsible for giving medicines that are ordered for the patient and should utilize
the EPOC device, which tests blood gas values — an important factor in diagnosing MH — in less than one minute. This final step can also be delegated to another nurse, if necessary.
• PACU charge nurse. The PACU charge nurse assigns a member of the PACU staff to be the recorder. They also alert pre-op and our second operating room about the crisis. We only have two operating rooms, so if there’s a surgery
in the other OR during an MH event, we want to make the other anesthesiologist is aware of the situation as well as check if there is another staff member available to help us. The PACU charge nurse can also call a manager and nurse leader
to inform them of the situation, plus delegate someone to retrieve bags of ice, which are needed to cool the patient and bring their temperature to within normal range. The goal is to stabilize the patient because they will soon be transferred
to our nearest hospital for continued care and observation.
The PACU charge nurse’s role is crucial because they must call 911 and designate someone from the front desk to keep an eye out for EMS responders who will be arriving to transport the patient to the nearest hospital. Finally, the PACU charge
nurse must also make sure someone from our anesthesia team, or the surgeon, has spoken to providers at the hospital about the MH crisis and the condition of the patient they are about to receive.
While most of the roles are slightly interchangeable, depending on if the MH crisis happens in the OR versus the PACU, there is one exception: The PACU charge nurse role. This is a role you want to stay the same so you can ensure the charge nurse
doesn’t have to worry about direct patient care during the MH crisis. Your charge nurse should stay behind the scenes, coordinating response efforts and positioning themselves to let the front desk know exactly when the emergency responders
are coming.
• Recorder. This person, who is a member of the PACU staff, is charged with procuring the EPOC device, and retrieving normal saline and insulin from refrigerated storage. The recorder must then grab the emergency response documentation
sheet, which is in the code cart, and record the following: the medications and fluids that are being used; the times various steps were taken (such as when medication was given, and when the Foley catheter or nasogastric tube was placed);
urine output as well as its color; and IV lines that have been inserted.
• Nurse assistant. This role’s primary responsibilities involve helping the circulating nurse with any of their tasks. For instance, the nurse assistant should ensure the placement of the Foley catheter, and receive the ice from
the PACU charge nurse and pack it around the patient. Finally, they should be the one to call the MH hotline (800-644-9737).
• Scrub tech. The scrub tech can assist in closing the case, clearing surgical equipment from around the patient and acting as a runner for equipment that’s needed during the crisis.
• Anesthesia tech. The anesthesia tech needs to grab a new soda-lime canister, breathing circuit and charcoal filter for the anesthesia machine. The goal is to stop the anesthesia machine from administering triggering agents, so you
want to replace the parts that have gas in them. The tech must also grab an esophageal temperature probe, a nasogastric tube and a Foley catheter, plus assist anesthesia in hanging extra IVs and tubing.
.svg?sfvrsn=be606e78_3)
.svg?sfvrsn=56b2f850_5)