.svg?sfvrsn=be606e78_3)

Communication is key as patients consult outside sources for information.
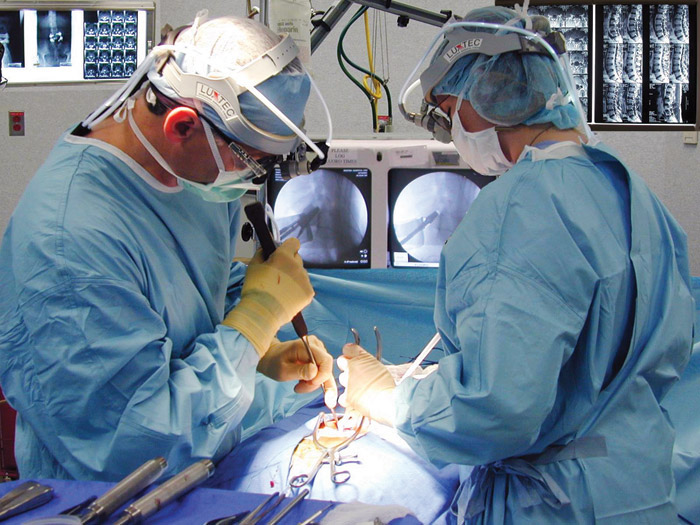
 Credit: Pamela Bevelhymer, RN, BSN, CNOR
Credit: Pamela Bevelhymer, RN, BSN, CNOR SAME PAGE Clinicians not only must communicate effectively with patients when predicting outcomes, but also ensure they are the patient's primary source of information.
Managing expectations is important in many walks of life, but perhaps none more so than in the world of surgery. That was the focus of a longitudinal investigation involving hundreds of patients by the Hospital for Special Surgery (HSS) in New York City that found surgeons should feel highly confident in the outcomes they predict for lumbar spine surgery, but they also need to make sure their patients are on the same wavelength.
HHS reported that surgeons' preoperative expectations were more accurate than patients' expectations in predicting patient-reported outcomes two years after lumbar spine surgery. The institution identified a related problem that led to this mismatch: "Most patients had higher expectations than their surgeons did, with many anticipating complete improvement after seeking additional information beyond that provided by their surgeons."
Federico P. Girardi, MD, an attending orthopedic surgeon at HSS, says that despite advances in spine surgery this century like minimally invasive and robotic approaches that have led to improved outcomes, patients' perceptions of the outcomes these procedures provide vary.
"Some patients report they are not doing well compared with others with similar conditions who received the same surgeries," says Dr. Girardi. "That has been very frustrating for surgeons because our goal is to optimize patient outcomes."
Carol A. Mancuso, MD, FACP, a general internist and clinical epidemiologist at HSS, adds, "Unrealistically high or low expectations are problematic, predisposing patients to poor outcomes if they become discouraged with recovery, abandon rehabilitation or ignore recommended lifestyle modifications that reduce disease progression."
As part of the HSS Lumbar Spine Surgery Expectations Survey, Drs. Girardi, Mancuso and others collected input from 402 patients over several years on the surgical outcome factors that matter most to them, exploring issues like symptom relief, resumption of activities and, in a new twist, psychological well-being, which previous surveys didn't capture.
They asked the patients and their surgeons to preoperatively assess their expectations of patient-reported surgical outcomes on a scale of 0 to 100, where a higher score indicates higher expectations. Two years after surgery, they surveyed patients again to evaluate their satisfaction. Surgical procedures ranged from a single herniated disc removal to more complex operations such as a five-level anterior-posterior decompression, instrumentation and fusion.
Patients' average preoperative score in the study was 73, with the surgeons at 57. Investigators then determined whose presurgical expectations more closely predicted postoperative fulfillment of those expectations, as reported by patients. In 73% of cases, surgeons either predicted patients' reported outcomes exactly or patients surpassed surgeons' expectations. Dr. Mancuso says the results show that HSS spine surgeons "very accurately" predicted patient-reported outcomes two years after surgery, adding the results show the surgeons' aptitude at integrating "complex clinical, surgical and psychological factors that matter most to patients."
One final finding shows how important effective patient-surgeon communication is for a patient's overall experience. HSS said 84% of patients had higher expectations than their surgeons, often expecting complete improvement. When they drilled down, investigators found many of those patients had "amplified" their surgeons' guidance with information they obtained from family, friends, coworkers and the internet.
"Our study underscores that there is room for improvement in patient education and that patients should rely on their surgeon's expertise when forming expectations of lumbar spine surgery," says Dr. Girardi. "Patients need to realize that anecdotal stories from social contacts or the internet are often not relevant to their situation."
.svg?sfvrsn=56b2f850_5)